
How can visually impaired people benefit from prismatic lenses?
According to the International Classification of Diseases 11 (ICD-11, 2019) vision impairment occurs when an eye condition affects the visual system and one or more of its vision functions. People with visual impairment often have partial or complete loss of visual perception, which manifests as a decline in visual acuity and/or visual field. That is why the term “low vision” is often used.
Counterintuitively, the health care improvement that we have witnessed in recent decades and the resulting increase in life expectancy have raised the number of visually impaired people. This happens because most eye diseases that cause vision loss are age-related, so their prevalence increases as more people enter the older population group.
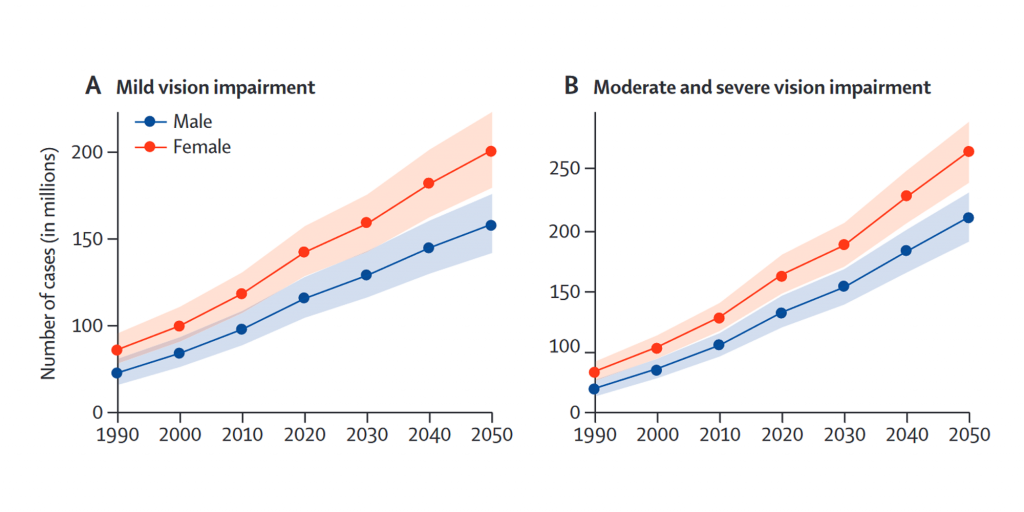
In fact, it is estimated that between 2020 and 2050, the world’s population older than 65 will double, growing from approximately 1 billion to 2 billion. This trend will have profound implications for age-related ocular diseases as can be observed in the projections in Figure 1.
When considering the entire world population, the most frequent causes of mild and moderate visual impairment are uncorrected refractive errors (especially presbyopia), cataracts, age-related macular degeneration (AMD), diabetic retinopathy, and glaucoma.
Refractive errors are easily addressed with modern ophthalmic lenses and surgical techniques for cataracts are increasingly effective in restoring good vision quality. However, it would be desirable that these technologies will become widespread in all countries. In contrast, other eye diseases such as glaucoma, age-related macular degeneration and diabetic retinopathy can easily cause permanent loss of visual function.
Scotoma and Preferred Retinal Locations (PRL)
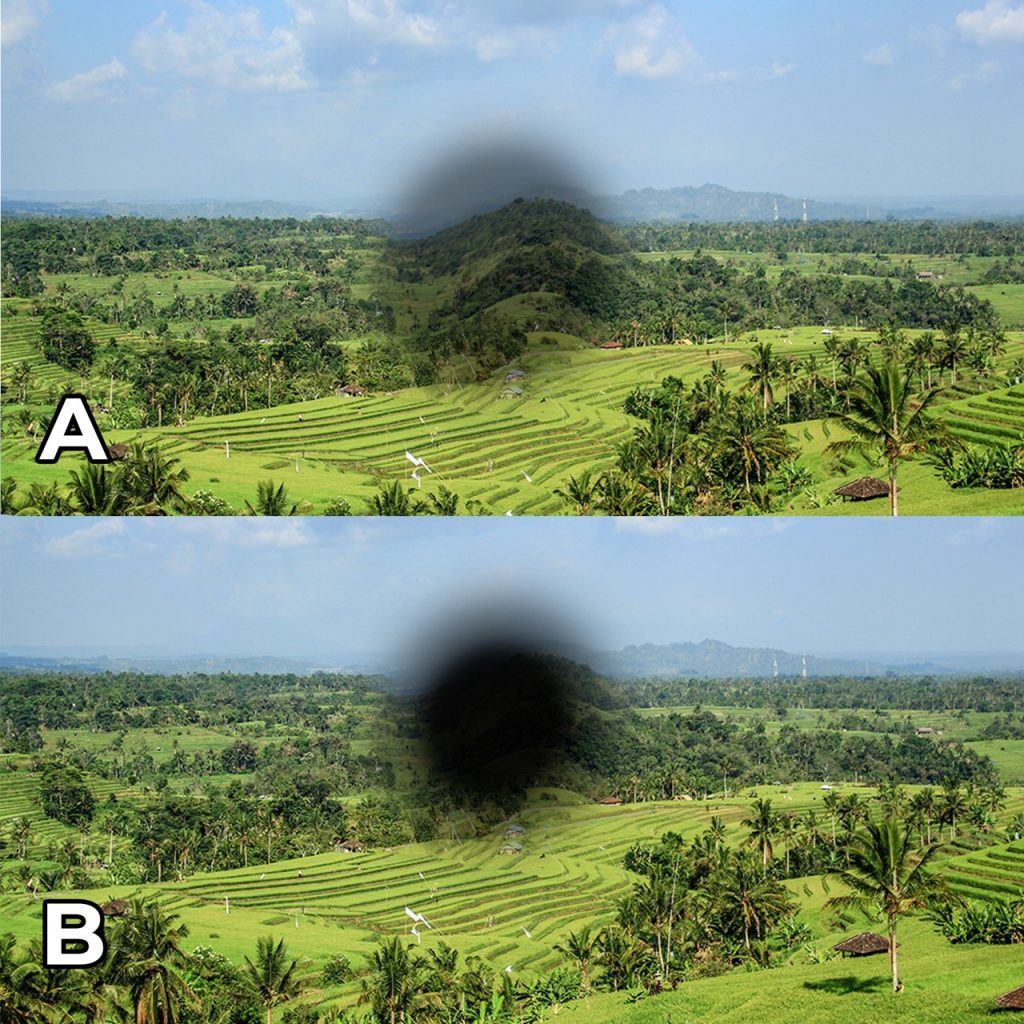
Degenerative eye diseases can completely or partially compromise portions of the ocular sensory tissue (the retina, located on the fundus of the eye-bulb). As a result, the person loses visual information from the involved retinal cells, either totally or partially. The corresponding compromised area of the visual field is called “scotoma”, and it is defined as “absolute” when visual information is permanently lost, otherwise it is called “relative scotoma” (Figure 2).
Some diseases, such as glaucoma, lead to a progressive loss of peripheral vision, eventually generating “tube” vision in more advanced stages. In contrast, other diseases (i.e., AMD) generate a scotoma in the center of the visual field, affecting the point of best visual acuity in the retina (the macula and more specifically the fovea).
In the latter case, visual acuity may be significantly reduced depending on the disease severity, and the person may have difficulty in object and face recognition, in reading and in many other daily activities.
Therefore, when the central scotoma is absolute and occurs in both eyes, the visual system chooses another spot on the retina to perform the central vision tasks with the purpose to “replace” the completely compromised fovea. This point is called the Preferred Retinal Locus (PRL) and the visual system reorganizes to use the visual information from the PRL cells for the fixation eye movement.
In most cases, the visual system independently develops a PRL in about 6 months after the onset of binocular absolute scotoma. If this process does not occur, visual rehabilitation techniques can be used to establish a PRL to improve residual visual acuity. When the person fully learns to fixate objects with the PRL, one can speak about “eccentric fixation”, as the eye fixation point is different from the retinal center.
How the visual system establishes PRL is a complex brain mechanism, and it is still a research topic. In addition, sometimes visually impaired people independently develop more than one PRL and they use one or the other depending on the activity they are doing. In this case, we speak of task-specific PRLs.
However, it can generally be said that PRL is established as close to the scotoma as possible to maximize visual acuity in the best eye and, in the worse eye, it is usually established in the corresponding retinal point of the other eye, to maximize binocular cooperation.
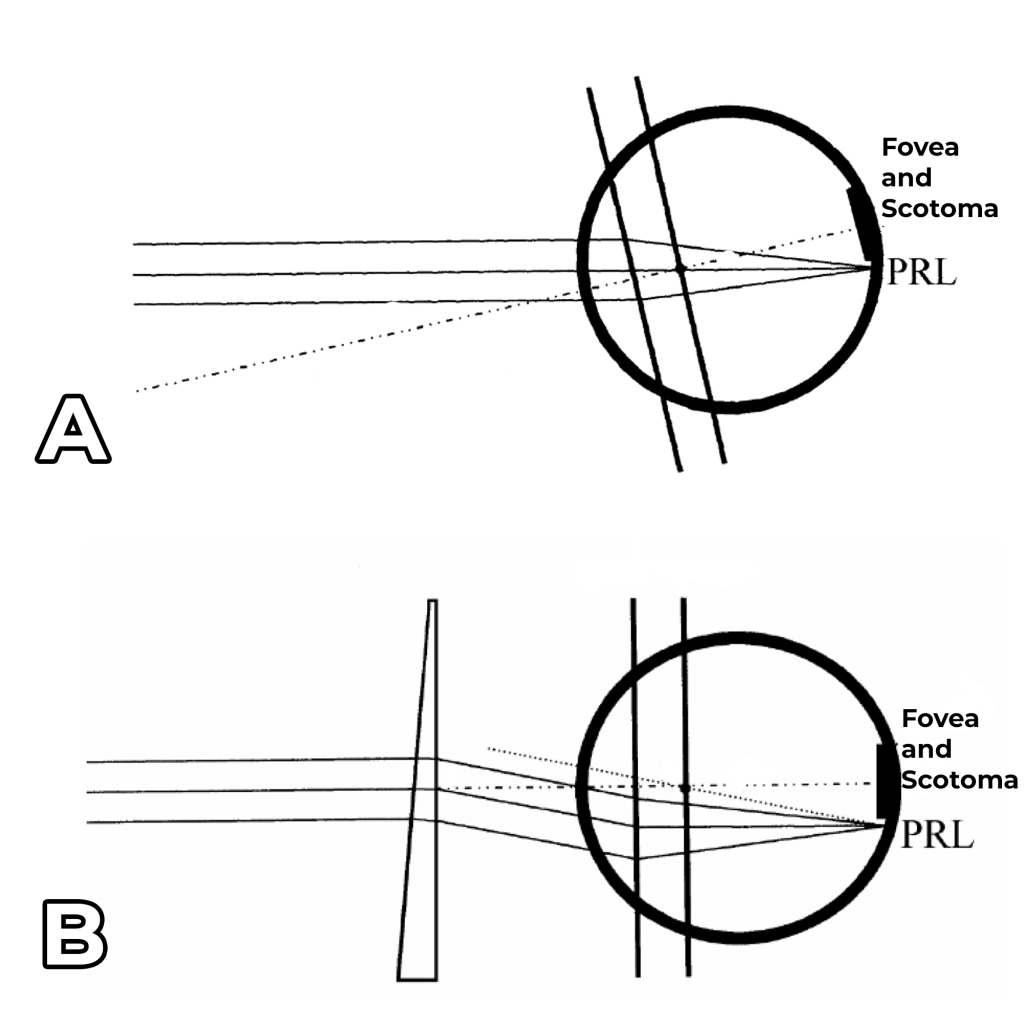
Prism lens in eccentric fixation
Eccentric fixation is therefore used in the presence of a central absolute scotoma in both eyes, and the PRL let the person benefit from a greater visual acuity compared to the compromised central vision. Thus, the person can overcome some barriers caused by the disease such as recognizing the faces of loved ones or distinguishing cutlery and food on the table.
However, while using eccentric fixation, you need to align the PRL with the observed object by performing an eye movement. Maintaining this fixation position can be bothersome and tiring, especially if the eye deviation is high or if you have to stare at something for a long time.
This is why in the 1980s it was proposed to use prismatic lenses to align the PRL with the observed object, to compensate for the ocular deviation required for eccentric fixation (Figure 3). Even from the early studies on the subject, there has been good acceptance of prisms in this use case; so, this practice has slowly become more and more common in low vision clinics.

These prismatic spectacles are often called Eccentric Viewing Spectacles (EVS) and more recent studies have found improved object search times, improved visual acuity compared to the compromised central vision, and higher scores on quality-of-life questionnaires.
In this use case, prisms must have equal power, axis and direction in both eyes, so they are called yoked prisms.
This is important to avoid binocular vision dissociation and, even if binocular vision is fragile or compromised, an attempt is made to preserve it as much as possible. In most cases EVS are used for distance vision and the best distance refraction is prescribed along with the prism. They are not widely used for near vision, probably because magnifying aids are more effective in improving reading (e.g., hyper-corrective prism glasses).
The most common prism values are 4 – 6 – 8 prism dioptres, although higher values can be found when diseases reach more advanced states, resulting in a bigger scotoma and higher ocular deviation. The prism axis is highly variable and depends on the size and type of scotoma and the consequent position of the PRL. As already mentioned, usually, it is a good practice to prefer the PRL of the better eye when choosing the prism axis (the eye with better visual acuity).
Furthermore, eccentric viewing spectacles also positively impact the visually impaired social life. In fact, the person who uses eccentric fixation may not feel comfortable showing the eye deviation (as for many cross-eyed people) or may be subject to social discrimination. Instead, wearing the EVS, which compensate for the eye deviation, the person can return to looking directly at the interlocutor during a conversation, using the primary gaze position again.
Despite the many benefits, in the past, many people often stopped using these devices because of the excessive weight and thickness of the lenses, which made the spectacles unesthetic and uncomfortable. Thanks to modern freeform optical surface calculation technologies, as the multi-aspherical automatic lenticularization algorithms developed by ProCrea Tech, it is now possible to drastically reduce the thickness and consequently the weight of these devices, aiming to reduce the drop-out probability and improve the quality of life of visually impaired people.
In addition, newer eccentric fixation lenses, developed in recent years, include a real image magnification of up to 7%, providing further visual acuity enhancement.
Conclusion
The number of visually impaired people is increasing and will continue to grow in the coming decades due to the age-related eye diseases such as AMD. It is possible to improve the visually impaired quality with the use of prismatic lenses when there is a central absolute scotoma in both eyes.
As the fovea is totally compromised, these people use a peripheral retinal point for central vision (called PRL) in an eccentric fixation position. Using glasses with yoked prisms, often referred as eccentric viewing spectacles (EVS), it is possible to compensate for the ocular deviation required for the eccentric fixation, improving visual comfort and quality of life of visually impaired people.
Modern technologies for freeform optical surfaces calculation, developed by ProCrea Tech, can significantly reduce the thickness and weight of these aids, improving EVS comfort and aesthetics. This could reduce dropouts, so more people will enjoy the benefits of EVS both on the visual function and on the psychological-social level.
References:
• R. Bourne et al., «Trends in prevalence of blindness and distance and near vision impairment over 30 years: an analysis for the Global Burden of Disease Study», The Lancet Global Health, vol. 9, fasc. 2, pp. e130–e143, feb. 2021, doi: 10.1016/S2214-109X(20)30425-3.
• J. D. Steinmetz et al., «Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study», The Lancet Global Health, vol. 9, fasc. 2, pp. e144–e160, feb. 2021, doi: 10.1016/S2214-109X(20)30489-7.
• World report on vision, WHO 2019.

Gaetano Volpe
Gaetano Volpe is a Computer and Automation Engineer. He’s a co-founder and Head of Research & Development at ProCrea Tech, freeform lens design company based in Italy. He’s pursuing a Ph.D. in Electrical and Information Engineering with the Polytechnic University of Bari. He has a long-time experience in optimization algorithms and lens design.

Pasquale Fanelli
Pasquale Fanelli is an optometrist from University of Salento. He works as product specialist for DAI Optical Industries, Italian ophthalmic lens manufacturer. He also practices as an optometrist in a private clinic and his fields of interest are freeform ophthalmic lenses and advanced contact lenses.
